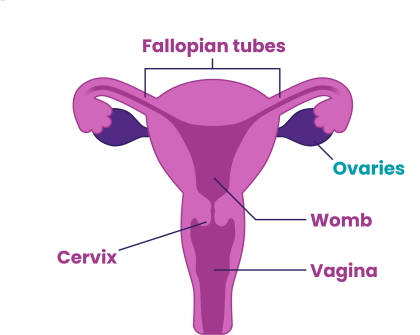
Epithelial ovarian cancer tumours start from the cells that line or cover the ovaries and fallopian tubes (the epithelium).
There are several different subtypes of epithelial ovarian cancer, which can behave and respond differently to treatment.
- High-grade serous
Sometimes known as high-grade serous carcinoma, this is the most common form of epithelial ovarian cancer. Over 6 in every 10 cases of epithelial ovarian cancer are high-grade serous.
Most high-grade serous ovarian cancers are now thought to start in the fallopian tube, not the ovary. So they may be classified as fallopian tube cancers.
This type of ovarian cancer is usually treated with a combination of chemotherapy and surgery, and generally responds well to chemotherapy.
- Low-grade serous
Sometimes known as low-grade serous carcinoma, this is a relatively rare form of epithelial ovarian cancer. 1 in every 10 cases of epithelial ovarian cancer are low-grade serous. These tumours are usually slow growing, and often detected in those who are younger.
Surgery is the most effective treatment for low-grade serous ovarian cancer, although chemotherapy and hormonal therapy are also used. These tumours respond less well to chemotherapy.
- Mucinous
Mucinous tumours make up a small percentage of ovarian cancers, at about three per cent (3 in every 100 cases). This type of ovarian cancer is usually treated with surgery with or without chemotherapy, but doesn’t respond as well to chemotherapy.
Mucinous tumours are categorised as:
- primary ovarian carcinomas (tumours starting in the ovary)
- metastatic from other sites (spread from somewhere else in the body, most often from bowels or stomach), which wouldn’t be classified as ovarian cancer.
Someone with mucinous cancer cells in the ovary often needs other tests. Colonoscopy or gastroscopy (a small camera inserted into the back passage or into the stomach) is used to rule out another primary cancer (a cancer that has started elsewhere in the body).
- Endometrioid
Ovarian endometrioid cancers may either be endometriosis-associated (developing from endometriosis) or non-endometriosis-associated. There's growing evidence these may be two different types.
In around a third of ovarian endometrioid cancers there may also be an independent separate endometrial (womb) cancer or endometrial hyperplasia (precancerous thickening of the lining of the womb). This type of ovarian cancer is usually treated with a mix of chemotherapy and surgery. Hormonal therapies such as Letrozole or Anastrozole (aromatase inhibitors – drugs that block oestrogen from being made), can also be used.
It's important to note that many more people have endometriosis than are diagnosed with ovarian cancer, so having endometriosis doesn’t mean you’ll develop ovarian cancer.
- Clear-cell
Clear-cell tumours, also known as clear-cell carcinoma, area rare tumour type making up four per cent of ovarian tumours (4 in every 100 cases of ovarian cancer).
Ovarian clear-cell carcinomas are still treated in the same way as other epithelial ovarian cancers with a combination of surgery and chemotherapy. They respond less well to chemotherapy.
- Undifferentiated or unclassified
Many epithelial ovarian cancers are known as unclassified or undifferentiated. This is because they have cells that are very underdeveloped and it's not possible to tell where they started to grow. These are usually treated with a combination of surgery and chemotherapy.
- Brenner tumours
Brenner tumours are rare, making up one to two per cent of ovarian tumours (1 or 2 in every 100 cases of ovarian cancer). They most commonly affect those over 40 years old.
Most Brenner tumours are benign (non-cancerous) and less than five per cent are borderline (slow growing) or malignant (cancerous). Surgery is the most common form of treatment for these tumours.
- Borderline tumours
Borderline tumours are a separate group of epithelial ovarian tumours, also known as tumours of low malignant potential. This means they are very slow growing and less likely to spread around the organs in the tummy. Even when they spread they don’t damage the tissues around them.
Borderline tumours are staged using the same FIGO/TNM system as ovarian cancers. They're usually treated by surgery alone.
- Carcinosarcoma
Carcinosarcomas are high-grade epithelial tumours that contain tissue that looks like both an epithelial cancer and a connective tissue cancer (a sarcoma). They behave like high-grade epithelial cancers and are treated in the same way with chemotherapy and surgery.
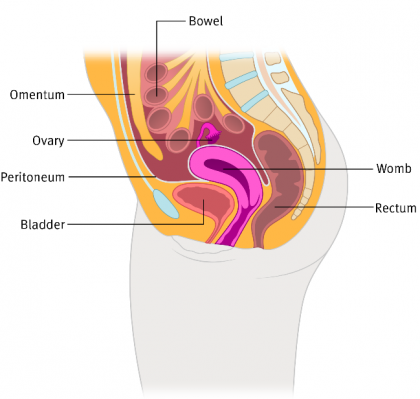
A note on primary peritoneal cancer
Primary peritoneal cancer (PPC) is similar to epithelial ovarian or fallopian tube cancer. It’s usually classed and treated in the same way. But PPC doesn’t start in the ovaries but in the lining of the peritoneum. This is a large, thin, flexible sheet of transparent tissue that covers the organs inside your tummy including your bowels, stomach, liver and reproductive organs. This means even those who have had their ovaries removed can develop this type of ovarian cancer.
Last reviewed: May 2022
To learn more about our review process, take a look at our information standards.
